Key messages
Workers in the healthcare and social assistance industry often work with people who are injured, unwell, experiencing mental illness or dementia, or experiencing other difficulties, such as the death of a loved one.
When people experience these things, they sometimes may behave aggressively. In some cases, this behaviour can be prevented from escalating through reducing stress and frustration in the workplace. In other cases, the person’s clinical condition may be contributing to this behaviour. This can become a hazard for workers and creates work health and safety (WHS) risks.
Workers in the healthcare and social assistance industry sometimes have to work with people who are behaving aggressively or displaying behaviours of concern. However, workers should never be harmed because of this.
As part of your primary duty to ensure the health and safety of workers at the workplace, you must do everything you reasonably can to protect workers from being harmed by violence, aggression and harassment at work. It may not always be possible for you to eliminate the risk of aggressive behaviour to workers. However, you must minimise the risk of people being injured by this as much as you can.
Jump to:
How you should identify and assess hazards and risks How you should control risks Case study: Gender-related violence in a hospital ward
Work-related violence, aggression and harassment are psychosocial hazards and fall into the group broadly termed ‘harmful behaviours’. They create risks of both physical and psychological harm to workers.
Note: Violence and aggression may happen between workers or come from other people at the workplace such as patients, clients, family members or the public.
Violence, aggression and harassment occurring between workers is covered in the section on psychosocial hazards.
This section is focused on work-related violence, aggression and harassment (including sexual harassment) from other people in the workplace, such as patients, consumers, clients, residents, family members or the public.
Healthcare and social assistance workers are particularly vulnerable to harmful behaviours due to high pressure, complex work environments and frequent interactions with people. When compared to other industries, the healthcare and social assistance workforce also has a higher proportion of female workers and workers from culturally and linguistically diverse backgrounds. This may increase the risk of some kinds of harmful behaviours, such as gender-based sexual harassment or racism. For more information, see the Code of Practice: Sexual and gender-based harassment.
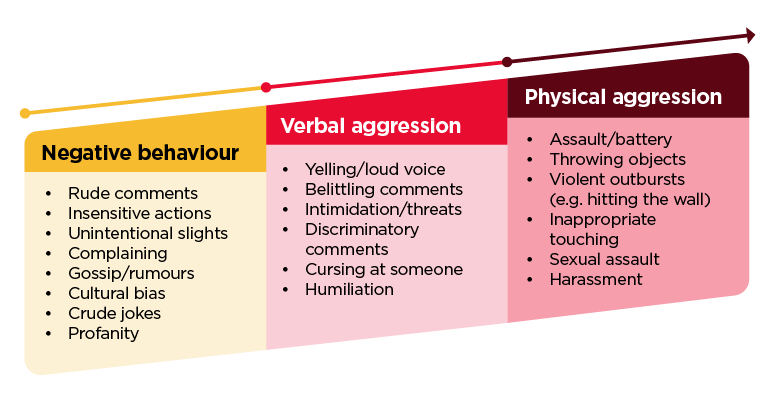
Subtle forms of violence, such as tensions between people, incivility, and rudeness, often lead to more extreme harmful behaviours when the causes of stress are not controlled. These subtle forms of violence can still be harmful, especially when they occur regularly or over a long time. The diagram below shows how behaviour can worsen over time if hazards are not controlled.
Figure 6: How harmful behaviours can worsen if not addressed early
You are responsible for protecting workers and others in the workplace from work-related violence, aggression and harassment (including sexual and gender-based harassment). You must eliminate risks if you reasonably can.
If that is not possible, you must minimise risks as much as you reasonably can.
For example, some consumers with psychiatric conditions may behave violently towards workers but still require medical treatment. In this situation, it may not be possible for an employer to eliminate the risk of violence to their workers.
However, employers must still minimise risks as much as they can (e.g. through effective medical management, placement in a specialised ward, having enough workers with the right mix of skills, having workers trained in de-escalation, having ‘code black’ arrangements, and, where required, the use of restrictive practices such as seclusion if risk cannot be effectively managed in another way).
The first step you must take is to do a risk assessment to work out what kind of risks their workers could be exposed to. The risk assessment should consider things like:
- if the work requires workers to deal directly with people
- how likely the violent behaviour is (e.g. do people being treated have medical conditions that may increase the chance of violence? Does the person have a previous history of violence? Could they be affected by drugs or alcohol?)
- the type of facilities available at a workplace (e.g. is there a safe place for workers to go if someone is behaving violently? Is there a lot of light and noise which may agitate people with certain conditions?)
These factors will help you understand the risk to workers. They must then use controls to prevent risks wherever they can.
To control the risks from harmful behaviours, you need to look at the underlying causes of the behaviour as well as addressing the behaviour itself. For example, harmful behaviours can be an inappropriate response to high levels of stress. While the behaviour itself should be addressed, if the cause of the stress is also not addressed, the risk will not be controlled.
For example, harmful behaviours from family members might result from:
- stress caused by long wait times without access to resources or information (e.g. updates on wait times and patient progress, lack of resources or amenities while waiting), or
- anger due to a perceived lack of fairness or concern and distress from thinking that their family member is not receiving the care they need.
Harmful behaviours may result from stress caused by:
- changes in work systems (e.g. sudden or unexplained shifts in daily routine, different personnel due to funding changes, work scheduling and staffing)
- anger due to a perception they are not being listened to or understood, or their needs not being addressed
- frustration (e.g. due to inattention or lack of active support, living arrangements or conflict with other residents)
- ability, or lack of ability, to make their own choices or have control
- withdrawal from medication, alcohol or other drugs, and
- use of restrictive practices as a last resort to prevent harm to a client or patient.
While you might not always be able to eliminate the sources of stress, there are a range of things you can do to minimise them, and therefore reduce the potential for violence, harassment, and aggression. Awareness of the sources will also help you to recognise early signs of an escalating situation and safely intervene.
In some cases, behaviour that is harmful to workers may not result from intentional aggression. Even when the harmful behaviour is not intentional, the WHS risks from the behaviour must still be managed by employers and contractors.
Work related violence is common to human services and care occupations in the healthcare and social assistance industry but has different causes and expressions in different types of workplaces. WHS controls should be sensitive to this (e.g. behaviours related to an intellectual disability are different to those related to dementia).
In some cases, it may be appropriate to remove the person displaying harmful behaviours, so they no longer pose a risk to workers. For example, a visitor who behaves aggressively may be:
- given a warning about the need to treat staff with respect
- issued with a barring notice limiting the times they can attend the facility (e.g. to times where there are additional workers or managers available, or when a particular worker is not on shift), or
- banned from the facility altogether.
How you should identify and assess hazards and risks
Consult with workers and others to identify and assess hazards and risks
How you should control risks
Consult with workers and others to design controls
Eliminate the risks of violence, aggression and harassment, including sexual harassment, as much as you reasonably can, including through good work design. Use the hierarchy of controls, particularly when seeking to reduce the risk of assaults.
Maintain and review controls to ensure they are being used and are effective, especially after any changes to the task or workplace.

Case study – Gender-related violence in a hospital ward
A 45-year-old male patient has just been admitted to a general ward with suspected early-onset dementia, as there were not enough spaces in the dementia ward to accommodate him. Throughout the day shift, nurses complain that he has been making frequent unwelcome comments, including sexual innuendo. The head nurse speaks to him about this behaviour, but the comments continue and escalate.
At the end of the day shift, this information is noted in the handover notes, but the shift handover is disrupted by a life-threatening emergency elsewhere on the ward, and ultimately not adequately discussed. A male nurse originally moved to the ward is diverted elsewhere due to competing patient needs.
At 3:00 am the next morning, a younger female nurse is asked to do rounds alone and the man assaults her.
The hospital investigates the incident and identifies multiple failures, including a lack of adequate staffing and worker training, a lack of consideration of the risk of escalation and violence, a failure to consider the gender mix of staff where there was an identified risk of sexual harassment, poor systems for information sharing and handover, and a lack of security systems and distress alarms for nurses. The hospital puts in place a range of changes to address these issues, which reduce the risk of a similar incident occurring in the future.