Key messages
Fatigue can be both a direct health risk to workers by itself and can also cause or contribute to other work health and safety (WHS) risks when workers become fatigued. Fatigue is often seen as ‘part of the job’ in the healthcare and social assistance industry. However, this is not the case, and you have a legal responsibility to eliminate or minimise the risk to health and safety from fatigue as much as you reasonably can.
In some industries, such as aviation, the risks of fatigue are well-recognised. Most people understand that a pilot must not fly a plane when they are too fatigued to do so safely. This same principle applies in the healthcare and social assistance industry. Workers, patients, and others in the workplace must not be put at risk of harm because a worker’s judgment or reaction times are impaired by fatigue. Likewise, your duty to manage the risks of fatigue are not removed by the need to care for patients, a worker’s preference for certain shift patterns, their willingness to work extra hours or to come to work when fatigued.
Jump to:
How you should identify and assess hazards and risks How you should control risks Case study: Fatigue in healthcare
Fatigue is an acute and/or ongoing state that leads to physical, mental or emotional exhaustion.
Fatigue can cause health and safety risks. It can directly harm workers (e.g. fatigue can cause heart conditions, musculoskeletal disorders, diabetes, high blood pressure and other health conditions). Fatigue can also impair judgment and slow reaction times, which may increase the risk of injuries, unless safety systems are in place.
For example, fatigue increases the risk of sharps injuries and medication errors.
Fatigue is more than feeling tired or drowsy. It can be:
- physical – pronounced physical exhaustion and a reduced ability to engage in physical activities (e.g. manual tasks or long or irregular working hours)
- mental – pronounced mental exhaustion and a reduced ability to engage in mental or cognitive activities (e.g. making complex decisions about patient care)
- emotional – pronounced emotional exhaustion and a reduced ability to engage in emotional activities (e.g. empathising with or caring for patients), or
- a combination of any of these.
Workers can become fatigued because of things that happen at work, outside of work (e.g. long hours of physically demanding domestic tasks) or because of a combination of work and non-work fatigue hazards. The way work is rostered and changed (e.g. constant and repetitive sleepover shifts, changes from night to day work) can also impact life outside of work for workers.
You must identify, understand and control fatigue hazards to prevent WHS risks.
Figure 5: How fatigue causes harm
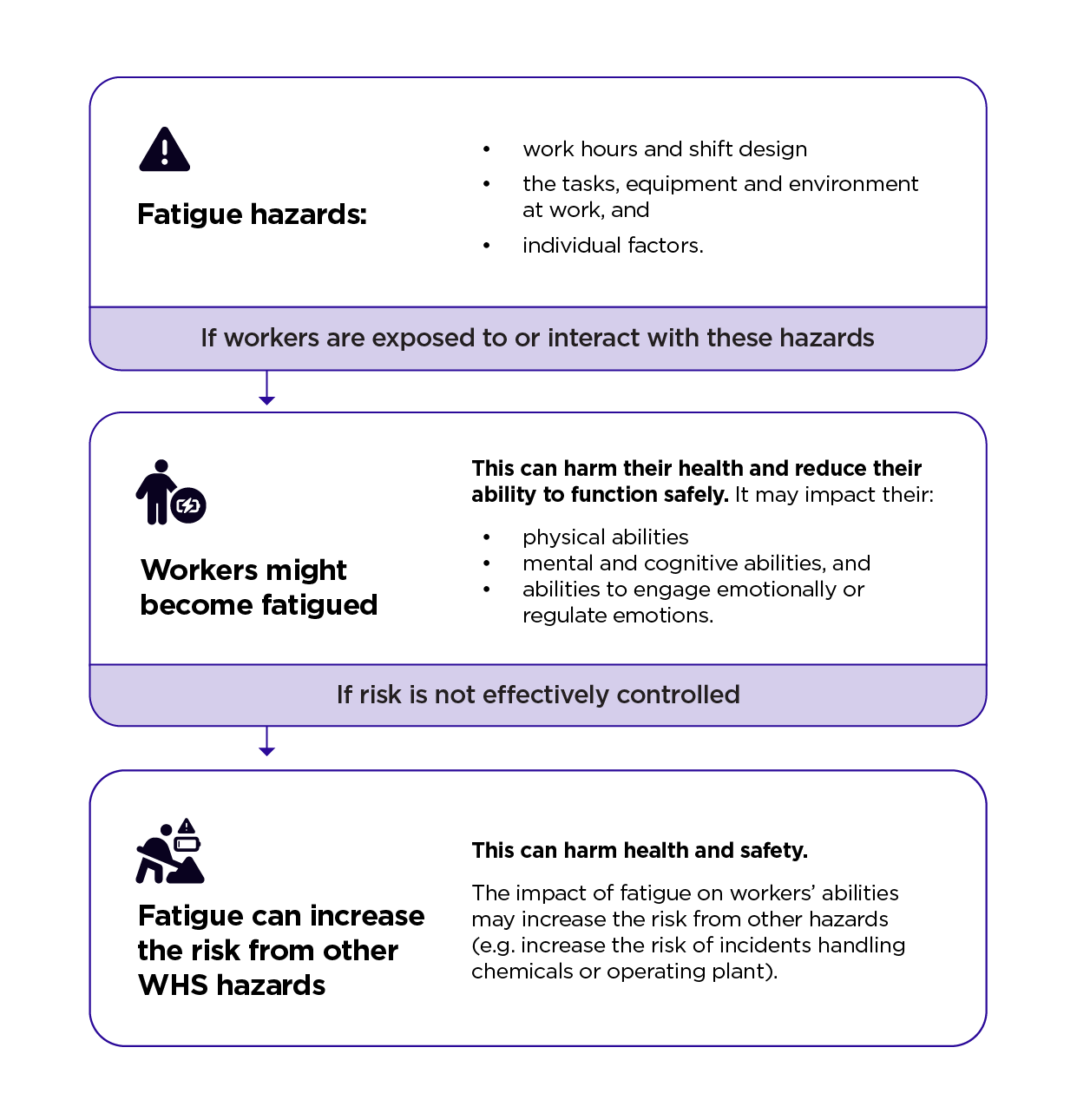
You must manage fatigue hazards at work by eliminating or minimising the risk of fatigue as much as you reasonably can. For example, you must:
- provide a safe work environment (e.g. install adjustable, low-vibration seats in vehicles, foster a culture where workers feel comfortable reporting fatigue)
- implement safe systems of work (e.g. by not allowing workers to work shifts that are too long, providing adequate breaks between shifts and rostering on enough people to do the work), and
- monitor workers’ health and the conditions at the workplace (e.g. by reviewing time sheets).
Your duties are not removed by a worker’s, or client’s, preference for certain shift patterns, their willingness to work extra hours or to come to work when fatigued. You have a duty to ensure workers, patients, clients or members of the public are not put at risk because a worker’s judgement or reaction times are impaired by fatigue (e.g. while performing surgery, checking medications or driving).
WHS responsibilities to manage the risks of fatigue do not mean workers can never work extra hours or multiple jobs. However, they should talk to their manager or supervisor about the risk of fatigue and avoid working arrangements that result in WHS risks.
Video courtesy of WorkSafe Victoria, 2025
Some fatigue hazards are common in the healthcare and social assistance industry (e.g. double shifts, being on call, frequent travel between clients or locations and doing physically, emotionally or mentally demanding work). Workers are more likely to become fatigued when exposed to a combination of fatigue hazards. Fatigue can be caused by a single instance of exposure to hazards, or over time with repeated or long-term exposure. Fatigue risks can be separated into:
- the risk of workers becoming fatigued which can directly cause health problems, and
- health and safety risk from fatigue-related incidents.
Rostering and staffing levels can significantly impact the risk of fatigue to workers. In the healthcare and social assistance industry, these factors may be determined by a client’s Support Plan. You may need to liaise with a client, their family, advocate, planner, navigator or guardian to ensure they have appropriate funding and support for workers to be rostered safely.
For more information, see the Managing WHS risks section and the Code of Practice: Managing the risks of fatigue at work.
Video courtesy of WorkSafe Victoria, 2025
How you should identify and assess hazards and risks
Consult with workers and others to identify and assess hazards and risks.
Examples of factors to consider when identifying fatigue risks:
How you should control risks
Consult with workers and others to design controls.
Eliminate the risks as much as you reasonably can by preventing workers from becoming fatigued, including through good work design.
If risks cannot be eliminated, minimise risks as much as you reasonably can. Consider the following example controls:
Many of the control measures to prevent fatigue can also help workers recover. For example, providing adequate time between shifts, increasing breaks and minimising job demands.
Maintain and review controls to ensure they are being used and are effective, especially after any changes to the task or workplace.

Case study – Fatigue in healthcare
After a medication administration error, a large city hospital conducted an investigation. The investigation found the nurse who made the error had worked more than 240 hours that month, including many long shifts of 10 hours at night and 12 hours in the day. The nurse had also worked night shifts at short notice to fill in for absent staff. The unit manager had not been able to call in replacement staff because of budget constraints. The nurse had also often worked shifts on backward rotation, and did not have 2 days off in a row for the entire month.
The investigation revealed there was no monitoring of the actual hours worked by staff, or consideration of whether they were too fatigued to do their job safely. Following the investigation report, the hospital developed a ‘safe hours’ policy with clear guidelines to minimise the risk of fatigue, including:
- a forward-rotating roster system
- a maximum number of night shifts that could be worked in a roster cycle
- a minimum number of days off in a roster cycle
- minimum break times between shifts
- escalation options for requesting replacement staff in certain situations
- monitoring and recording of actual hours worked, and
- monitoring of staff fatigue, and procedures for reporting this.